What is Pre-implantation Genetic Testing for aneuploidy (PGT-A)?
Pre-implantation genetic testing for aneuploidy (PGT-A) is the procedure where a few of the cells of the embryo are removed and the chromosome content of that embryo is analysed to determine whether the amount of genetic material is normal or abnormal. By excluding the abnormal embryos during fertility treatment, the procedure should theoretically increase the chances of a successful pregnancy. PGT-A helps to prevent possible transfer of embryos which would end up not implanting, miscarrying or proceeding onto abnormal birth. However, this screening may also result in no embryos being found that are normal so no transfer can take place.
PGT-A is a selection tool to increase the likelihood of a healthy on-going pregnancy and is not a guarantee of pregnancy. The only way to create embryos for PGT-A is through IVF or ICSI treatment. You will be given specific information regarding your treatment protocol which will be identical to any patient undergoing IVF/ICSI treatment to create embryos.
What are chromosomes?
Chromosomes are minute, rod-shaped structures that exist in virtually every cell in the body. Each embryo should have exactly 46 chromosomes; 23 come from the egg and 23 come from the sperm. The chromosomes carry the genes, which are the chemical instructions that tell the embryo how to develop into a baby. The genes could be thought of as being blueprints.
What happens if an embryo has an incorrect number of chromosomes?
Research has shown that many embryos have an incorrect number of chromosomes in their cells, a condition known as aneuploidy. If a chromosome is lost, or if one of them is duplicated, the genetic instructions no longer make sense and the embryo will be unable to form a healthy baby. Most abnormal (aneuploid) embryos fail to implant in the uterus or miscarry during pregnancy. However, there are very few cases where a pregnancy can reach full term and a baby is born e.g. Down’s Syndrome.
In some cases, an embryo with the wrong number of chromosomes will spontaneously stop growing during its development in the laboratory and will not form a blastocyst (day 5/6) stage embryo. These embryos would not normally be considered for transfer. However, the majority of aneuploid embryos will not stop growing until they have been transferred into the uterus. The major difficulty faced in the laboratory is that they are indistinguishable from their normal counterparts judging by their appearance alone. There is a risk that an aneuploid embryo would be recommended for transfer instead of a normal embryo, which may explain some unsuccessful IVF treatments.
How common are chromosome abnormalities in embryos?
It has been shown that the risk of chromosome abnormalities is greatly influenced by the age of the mother. For women in their early thirties, about 35% of embryos are abnormal. However, over the age of 40 it is typical for at least 75% of embryos to suffer from aneuploidy.
The next table shows a recent study, analysing a large number of PGT-A cycles throughout the world, and it gives statistics on the chances of having one normal embryo when performing PGT-A. For example, if you are between 38 and 40 years old and have 1-3 blastocysts available to biopsy, there is a 60% chance you will have at least ONE normal embryo. That, in turn, means that 40% of patients will not have a transfer as no normal embryos are available.
These statistics are used as a guide for you only.
| Number of blastocysts | % of patients with at least ONE normal embryo
N = 3,571 cycles and 19,356 embryos, up to 8/2013. |
|||||
| Egg donors | <35 years | 35-37 years | 38-40 years | 41-42 years | >42 years | |
| 1-3 | 86% | 85% | 72% | 60% | 58% | 24% |
| 4-6 | 95% | 97% | 95% | 88% | 69% | 54% |
| 7-10 | 100% | 99% | 96% | 92% | 85% | 65% |
| >10 | 100% | 100% | 98% | 98% | 92% | 83% |
Are the chromosomes of embryos routinely tested?
In most cases the answer is ‘No’. In the IVF laboratory, the embryologist will look at the embryos down the microscope and grade them based on their physical appearance (morphology). The assumption is that the better the appearance, the better the quality of the embryo and hence more likely to implant. The only way of looking at the chromosome content of the embryo is by performing a biopsy of the cells and doing a PGT-A test.
What is PGT-A?
PGT-A or pre-implantation genetic testing for aneuploidy are tests that can be performed, where some cells are taken from the embryo and sent for analysis to count the number of chromosomes. Embryos with a normal number of chromosomes can therefore be selected for transfer, and are thought to give a higher chance of creating a healthy baby. There is, however, a risk that no embryos will progress to the stage for biopsy, or no embryos will have a normal number of chromosomes and no transfer will be performed.
In the UK and in Greece, it not legal to use this testing to select embryos on the basis of their sex for social/family balancing reasons.
Who is PGT-A suitable for?
PGT-A is recommended to those couples that have a greater likelihood of having a chromosome problem in their embryos, as they are most likely to benefit.
These are:
- Couples with a history of recurrent miscarriages
- Couples who have had several failed IVF attempts
- Couples who have had previous pregnancies affected by chromosome abnormalities
- Women over the age of 36
Theoretically, PGT-A may reduce these risks, although this has not been conclusively proven. Overseas clinics have begun to offer PGS to all patient groups, outside of the above criteria, to help improve outcomes.
Studies into PGT-A
Many years ago, the PGT-A test was performed by a technique called FISH (fluorescent in situ hybridisation), which only looked at limited number of chromosomes in the embryo. These early studies were not effective at increasing the likelihood of a live birth. Technology has since improved and the genetics lab are now able to use tests that detect all of the chromosomes and are therefore more effective.
Recent studies using these new techniques showed that the chances of an embryo with a normal number of chromosomes producing a baby was more than 25% higher than those chosen based on the look of the embryo (morphology). While these results are extremely promising, they have not yet been replicated by other IVF centres. There needs to be further robust clinical and laboratory trials to assess whether or not PGT-A can significantly increase live birth rates. These studies are currently being performed. Although there are studies reporting improvements in IVF success rates using PGT-A, there is other research suggesting that chromosome testing is of no benefit. There is also data suggesting that PGT-A may be of no benefit to patients with less than 3 embryos suitable for biopsy, although this is always a discussion the Consultant will have with you on the day of biopsy.
What is involved in PGT-A?
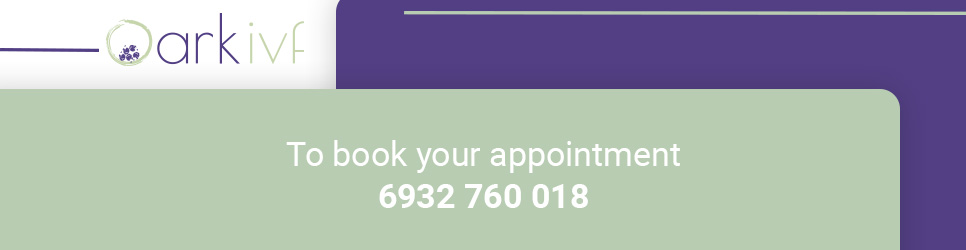
PGS can only be performed when embryos are created via IVF. This involves stimulation of the ovaries, collection of eggs, fertilisation and culturing of embryos to day 5. On day 5 (or sometimes day 6), embryos will be assessed and those that have made a suitable blastocyst can be biopsied by a highly-skilled embryologist in a state-of-the-art genetics laboratory. Between 2 and 5 of the trophectoderm (TE) cells are removed from the blastocyst. These cells are known as ‘extra-embryonic’ and produce tissues such as the placenta.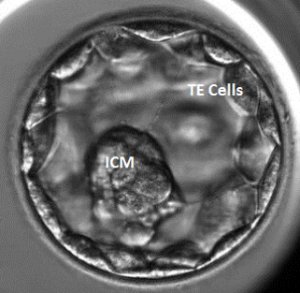
There are over 100 trophectoderm cells in a blastocyst so the removal of very few of these cells rarely impacts on the embryo. Testing these cells can then give a prediction of whether or not the embryo has a normal set of chromosomes. The inner cell mass (ICM) is the group of cells that would produce the potential fetus.
Straight after the biopsy procedure the embryos will be frozen to await the results of the test. There will be no transfer of embryos in that cycle unless you no longer wish to have the PGT-A testing and remove consent prior to embryo biopsy. If a normal embryo is identified after the testing then these will be given top priority for transfer in a frozen embryo replacement cycle (FER).
Patients electing to proceed with PGT-A will have their embryos cultured to blastocyst stage regardless of quality on day 3. If embryos do not reach the blastocyst stage then it is most likely these embryos are aneuploid (abnormal) and unlikely to result in a successful pregnancy. Embryos that do not reach a suitable blastocyst stage cannot be biopsied for technical reasons. Embryos that are slower to develop into a blastocyst can be cultured on to day 6 and if they reach a suitable stage can be biopsied then.
 |
 |
 |
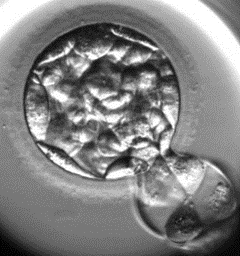 |
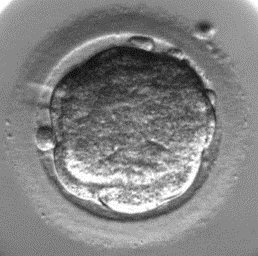
| 1. Morula | 2. Starting to cavitate | 3. Cavitating | 4. Full blastocyst |
These are pictures of developing blastocysts; they show the very early stage (Morula), then the central cavity is slowly filled with fluid (2 and 3). These stages (1-3) are too early for us to physically take any cells, however when the embryo reaches the full blastocyst stage (4), we would be able to proceed with the biopsy. At any point patients can elect to proceed with an embryo transfer without biopsy.
Abstaining from unprotected intercourse during IVF treatment
It is critical that patients avoid sexual intercourse or use barrier contraception from the down-regulation blood test until the pregnancy test. This is required because sperm can survive up to 15 days after intercourse, it is therefore possible that sperm from intercourse may fertilise a retained egg and this may result in the implantation of an untested embryo. This would negate the results of the PGT-A test.
Test results and accuracy
The main test that is offered by our collaboration genetics laboratory is NGS (Next Generation Sequencing). It analyses the entire set of chromosomes of the embryos. NGS has a lower cost than traditional methods and is also able to detect mosaicism (where some cells have different chromosome numbers to other cells in the same embryo).
A report is then generated and is sent to your doctor, who will contact you as soon as the report is received. This is usually 2-4 weeks after the biopsy procedure.
In most cases, some embryos will be normal and some will be abnormal. However, as explained previously, there is a chance that none of the embryos will be normal, in which case there will be no embryo transfer.
Additionally, less than 5% of embryos tested will fail to give a result. This can be due to the chromosomes degrading before testing, or technical errors. Embryos without a result can still be transferred, but it will not be possible to say whether or not they have a correct number of chromosomes.
These tests will only look at the numbers of chromosomes in the embryo and cannot detect genetic disorders. If either partner carries a specific genetic disorder that could impair the normal development of a child affected by the disorder, you will be referred for PGD (pre-implantation genetic diagnosis). In turn, PGT-A cannot screen against genetic disorders and does not guarantee a child will not be born with a genetic disorder (e.g. Cystic Fibrosis) rather than a chromosomal disorder (e.g. Down’s Syndrome).
Results of PGT-A
It typically takes 4 weeks to receive the test results from the genetics laboratory. You will be telephoned by your doctor, who will discuss the results and send you a summary letter. If there are normal embryos then the next stage is to arrange the Frozen Embryo Replacement (FER) Cycle. If there are no normal embryos you may wish to arrange a medical review.
Booking for Frozen Embryo Replacement (FER)
Once the results of the PGT-A testing have been received, if there are any embryos suitable for transfer then the embryologist will inform the nursing team to arrange for the FER cycle. You will then be given specific information regarding your FER treatment protocol.
If there are no embryos suitable for transfer you will be offered a consultation with your doctor to discuss the cycle and the future treatment options for you. Legally the team will also need your consent to allow the abnormal embryos to perish.
Antenatal Screening
PGT-A is a ‘pre-implantation’ test, which carries a small risk of misdiagnosis. Therefore, if you do become pregnant, conventional ‘prenatal’ cytogenetic analysis is still highly recommended. The intention of the PGT-A is to decrease the risk of transferring an embryo with loss or gain of whole chromosomes. However, technical limitations mean that the detection and transfer of a chromosomally normal embryo cannot be 100% guaranteed, though the risk of misdiagnosis is less than 1%.
Chorionic villous sampling (CVS), amniocentesis and ultrasound scans are used to confirm the chromosome content of the pregnancy. Non-invasive prenatal test (NIPT) can also be used which is a blood test in early pregnancy. This however, only detects 5 chromosomes so is not as comprehensive as PGS or standard CVS/amniocentesis tests.
Risks of PGT-A
As with all artificial reproductive techniques, it is important to understand the risks that are involved when using these tests. Below is a list of the potential risks for you to consider before embarking on IVF with PGT-A.
Risk of an unsuccessful outcome and miscarriage
Performing PGT-A and having a normal embryo transferred does not, unfortunately, guarantee a positive pregnancy test, a viable early scan or a healthy live birth. PGS has large financial and emotional costs and counselling is available for either partner at any stage of treatment should you wish.
As with all pregnancies there is also a risk of miscarriage. PGT-A testing and replacement of a chromosomally normal embryo does not eliminate the risk of miscarriage; it can only serve to reduce the risk.
Risk of the cell biopsy procedure
It is currently unknown whether embryos derived from biopsied embryos have the same likelihood of implanting as embryos from unbiopsied embryos. The procedure of removing the cells (biopsy) may lower the implantation rates in the absence of a PGT-A result, but selection of normal embryos via PGT-A may more than compensate for any negative effect of biopsy.
If an embryo is damaged by the procedure, it may not produce an embryo suitable for transfer. The risk of damaging an embryo is less than 1%. Worldwide several thousand babies have now been born from IVF with PGT-A, with no reported increase of congenital abnormalities above the general population rate of 3-5%.
Risk of preparation of biopsied cells
After the biopsy procedure, the cells are placed in a small test tube for their testing. The cells are no longer viable in any way after this process and can only be used for PGT-A. A fraction of the cells may not yield a test result (<5%), some may not contain any genetic material, cells may be lost during the highly technical fixation process of the test, or may have suboptimal fixation rendering it inadequate for the complex analysis.
Risk of misdiagnosis
Misdiagnosis can result in false positive results (normal embryos being diagnosed as abnormal) or false negative (abnormal embryos being diagnosed as normal). The risk of clinical misdiagnosis is less than 1%. Due to the chance of misdiagnosis, we strongly recommend prenatal testing.
Risk of having nothing available for biopsy
As discussed before there is a chance that no embryos will be suitable for biopsy as they haven’t reached the correct stage of development. In these cases, it is highly likely that the embryos that have stopped developing are chromosomally abnormal and would not produce a viable pregnancy.
Risk of no normal embryos
The test may find that none of the embryos are normal, in which case there may be no embryo transfer procedure. The likelihood that this will happen is influenced by a variety of factors; mainly female age and the number of embryos.
Risk of no diagnosis/partial diagnosis
Some embryos may have no diagnosis, due to the absence of chromosomes, or technical difficulties in the fixation process. Embryos without a result can still be transferred, but the possible advantages of PGS will not apply. In addition, sometimes the analysis may not be clear for one of the chromosomes tested. Embryos with such partial results may be transferred, but this must be discussed with either a geneticist or a consultant. The risks of transferring such an embryo will be explained to you.
Current PGT-A techniques are unable to provide a 100% guarantee that the child will have a normal set of chromosomes after IVF and PGT-A.
Alternatives to PGT-A
Alternatives to PGT-A during pregnancy include standard prenatal testing for abnormalities (chorionic villous sampling – CVS, amniocentesis, ultrasound examination). These methods will identify pregnancies affected by abnormalities such as Down’s syndrome, but not increase the chances of a successful IVF cycle. You are not obliged to undergo PGS even if your consultant recommends it.
Another newer test available is the Non-Invasive Prenatal Test (NIPT), which is a simple blood test, which can detect 5 of the most common chromosome abnormalities. This is done in early pregnancy but again does not increase the chances of a successful pregnancy. If these tests come back with an abnormality then this will be discussed with you further and you may wish to terminate the pregnancy. You will be fully counselled should this happen.
Confidentiality
Confidentiality of your records will be maintained at all times. Only personnel of the reference laboratory will have access to your records.
Counselling
At all stages of your treatment cycle, you have access to an independent counsellor. Should you wish to book an appointment, please call the main clinic number and this can be booked for you. The counsellor does not have any access to your clinical records and will not disclose any information that you discuss with them.